Introduction (Terminology):
Testicular atrophy, or testicular atrophy, is characterized by a significant decrease in the size of the male gonads. This leads to a significant decrease or complete cessation of testosterone and sperm production, causing androgen deficiency and, as a result, male infertility. In most cases, testicular atrophy is an irreversible process.
Key indicator: the volume of the affected testicle decreases to 6 cubic centimeters or less, which contrasts with the average volume of a healthy organ of 17-18 cubic centimeters. It is important to note that there are reversible conditions, such as subatrophy or hypotrophy, in which testicular function is only partially reduced. The severity of the damage affects the recovery potential.

Now about the most important thing, especially for those who are involved in bodybuilding and take steroids - steroids and hormonal imbalance:
Abuse of anabolic steroids and prohormones is one of the main causes of testicular atrophy in athletes. External steroid hormones suppress the body's natural testosterone production.
How it works:
- The hypothalamic-pituitary-testicular (HPT) axis is the system that regulates testosterone production. The hypothalamus releases gonadotropin-releasing hormone (GnRH), which stimulates the pituitary gland to produce luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH, in turn, stimulates the Leydig cells in the testicles to produce testosterone.
- Feedback (aka feedback mechanism). Testosterone has a negative feedback effect on the hypothalamus and pituitary gland, reducing the production of GnRH, LH, and FSH.
- Steroids and HPTA suppression. When exogenous steroids enter the body, the hypothalamus perceives this as excess testosterone and reduces the production of GnRH. This leads to a decrease in the production of LH and FSH by the pituitary gland.
- Cessation of testicular stimulation. ET means that without sufficient stimulation of LH, the Leydig cells stop actively functioning and producing testosterone. The testicles, deprived of the necessary stimulation, gradually decrease in size.
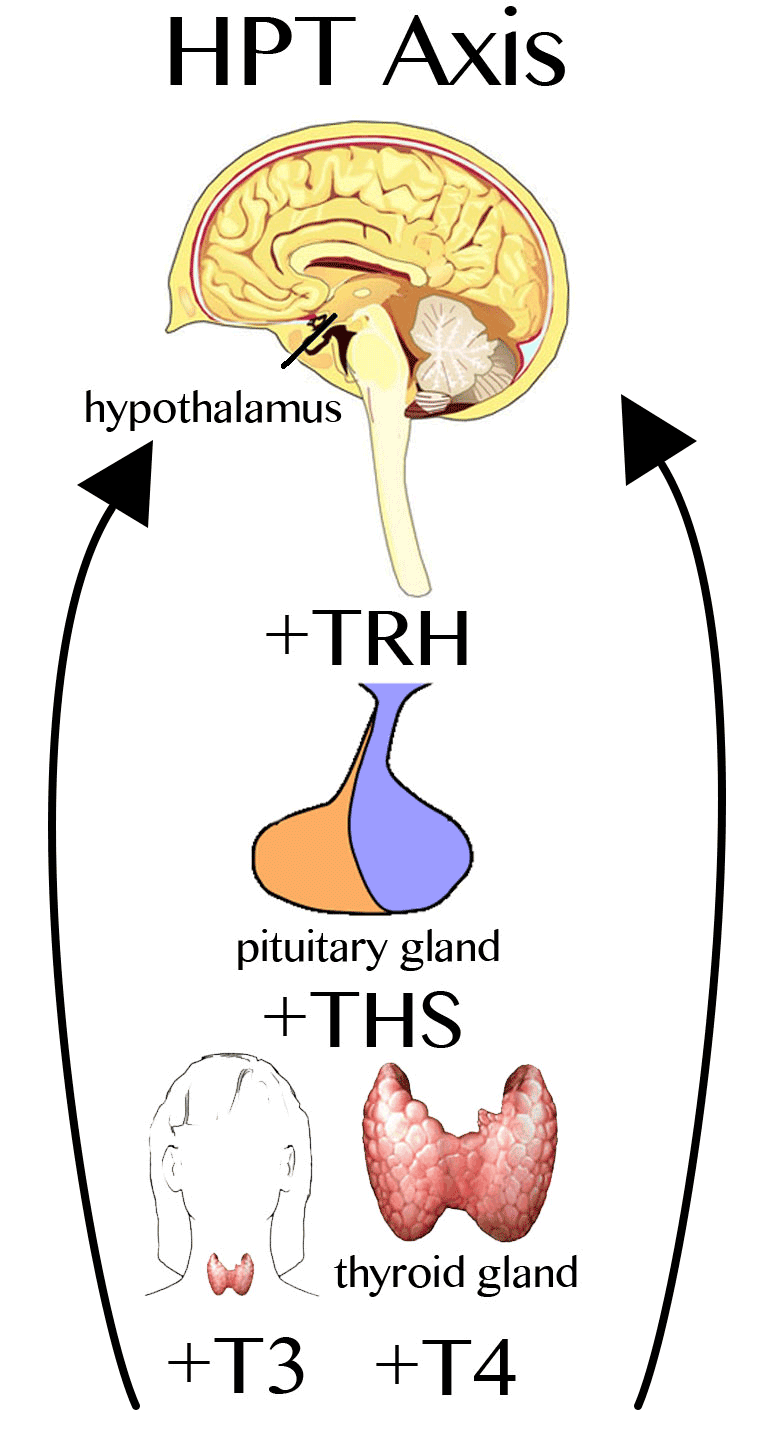 HPT Axis
HPT Axis
Important information:
- The longer and in larger doses steroids are taken, the more the HPTA axis is suppressed and the higher the risk of testicular atrophy.
- After stopping steroid use, recovery of testicular function may take a long time, and in some cases may be incomplete or impossible.
- It is important to remember that recovery after taking steroids is a long process that requires medical intervention.
What to do to minimize the risks:
- Avoid steroid abuse. The most effective way to prevent testicular atrophy is to avoid taking steroids.
- Consult a doctor. If you are planning to take steroids, be sure to consult a doctor to assess the risks and get recommendations on how to minimize side effects.
- Follow the dosage and duration of the course. If you do take steroids, strictly follow the recommended dosage and duration of the course.
- Perform post-cycle therapy (PCT). After completing a course of steroids, it is necessary to perform PCT to help restore natural testosterone production.
- Get regular check-ups. Get regular check-ups with an endocrinologist to monitor testosterone levels and other health indicators.
This article will help you make informed decisions and take care of your health. And for those who are already on the course and are somehow worried and worried about their future (well, you get the idea), we will give advice on how to smooth everything out.
Regulation of Testicular Function: The HPTA Axis and the Effects of Anabolic Steroids
The testicles play a key role in the male reproductive system, responsible for the formation of germ cells (spermatogenesis) and the production of androgens, primarily testosterone. Testosterone, a 19-carbon steroid, is the major androgen in most mammals and is vital for maintaining sexual function, germ cell development, and secondary sexual characteristics. It also affects muscle and bone tissue, hematopoiesis, blood clotting, lipid metabolism, carbohydrate and protein metabolism, and psychosexual and cognitive functions. During fetal development, testosterone ensures masculinization and the formation of external genitalia. During puberty, it stimulates growth and virilization in boys.
The hypothalamic-pituitary-testicular (HPT) axis is a key regulator
Testicular function is tightly controlled by the HPTA axis, a complex hormonally interconnected system that includes the hypothalamus, pituitary gland, and testes themselves.
- Hypothalamus: Secretes gonadotropin-releasing hormone (GnRH), which stimulates the pituitary gland.
- Pituitary gland: In response to GnRH, releases luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
- Testes: LH stimulates the Leydig cells in the testes to produce testosterone. FSH, together with the high concentration of testosterone inside the testes, is necessary for normal spermatogenesis. Sertoli cells, interacting with germ cells, also play an important role in regulating spermatogenesis.

Mechanisms of regulation:
Testicular function is regulated by a complex feed-forward and feedback system that operates at the level of the hypothalamus, pituitary gland, and the testes themselves.
- Direct stimulation. The wave-like secretion of GnRH stimulates the production of LH and FSH.
- Feedback. Sex hormones, including testosterone, estrogens (formed from testosterone by aromatase), as well as inhibin and activin, regulate the secretion of GnRH, LH, and FSH.
Effect of anabolic steroids on the HPTA axis
The use of exogenous anabolic steroids has a significant effect on the HPTA axis, leading to the suppression of natural testosterone production.
Exogenous steroids, especially estrogens formed because of aromatization of some steroids, suppress the production of GnRH in the hypothalamus and, as a result, reduce the secretion of LH and FSH by the pituitary gland.
Regarding the decrease in stimulation of the testicles, the decrease in LH production leads to a decrease in stimulation of Leydig cells and a decrease in testosterone production.
A decrease in spermatogenesis can also be observed. A decrease in FSH and testosterone levels disrupts the process of spermatogenesis.
Key points:
- It is estrogens, not testosterone, that have the main suppressive effect on the HPTA axis when exogenous steroids are administered.
- Long-term and uncontrolled use of anabolic steroids can lead to irreversible changes in the HPTA axis and decreased fertility.
- Post-cycle therapy (PCT) is aimed at restoring the normal function of the HPTA axis after steroid use is stopped.

Main Signs of Testicular Atrophy and Subatrophy: How to Recognize the Problem
| № | Sign | Description |
| 1 | Bilateral decrease in testicular volume. | This is one of the most obvious signs. However, it is important to remember the nuances that I will discuss below. |
| 2 | Symptoms associated with testosterone deficiency. | Decreased testosterone production manifests itself in a number of symptoms affecting various aspects of life. |
| 3 | Feminization | the appearance of feminine traits, such as enlarged breasts (gynecomastia). |
| 4 | Changes in sperm. | Decreased sperm volume and decreased sperm count and quality (oligospermia, azoospermia). |
Also note a few more symptoms below:
- Deterioration of general well-being and decreased performance.
- Decreased mood, apathy, depressive states.
- Decreased libido (sexual desire) and impaired potency.
- Decreased desire and willingness to train, deterioration in athletic performance.
- Loss of muscle mass and strength.
Important diagnostic nuances:
Leydig cells, responsible for testosterone production, make up only about 5% of the total testicular mass. Therefore, even with a significant decrease in the function of these cells, the change in testicular size may be minimal and imperceptible upon palpation. Palpation analysis of testicular size is not a reliable method for assessing the loss of Leydig cells, since the volume can change very slightly (by only 5%) with almost complete suppression of function.
The loss of spermatogenesis cells is more noticeable upon examination and palpation; the loss of these cells significantly reduces the volume of the testicles.
What is important to consider:
Diagnostics of testicular atrophy/subatrophy require a comprehensive approach, including:
- Examination and palpation of the testicles.
- Blood test for hormones (testosterone, LH, FSH, estradiol).
- Spermogram (sperm analysis).
- Ultrasound of the testicles (if necessary).
Dear athletes, if any signs of testicular atrophy/subatrophy appear, you should consult an endocrinologist or urologist for diagnosis and treatment.
Treatment (and prevention) of testicular Atrophy: How to Protect Men's Health
The main tool for preventing testicular atrophy when using anabolic steroids is the use of human chorionic gonadotropin (hCG). hCG is available under various trade names (Novarel, Ovidrel, Pregnyl, Biogonadyl, chorionic gonadotropin, Pregnyl, Profasi, Choragon and others).

Human Chorionic Gonadotropin: Basic Information
The use of hCG (human chorionic gonadotropin) during an anabolic steroid course is, in essence, an attempt to support the testicles and prevent them from «fading.» And although this is a common practice, it is important to understand that there is no universal scheme here, everything is very individual. The choice of protocol depends on how long the course lasts, what drugs are used, and how your body reacts to all this in general.
An interesting fact about the mechanism of action of hCG: hCG mimics the action of luteinizing hormone (LH), stimulating the Leydig cells in the testicles to produce testosterone. This helps prevent testicular atrophy by maintaining their function during the steroid course.
When to start taking hCG?
If you are taking a strong course of steroids, it is recommended to start using hCG as early as 2-4 weeks of the course to prevent the development of testicular atrophy. If the course is short, from six to ten weeks, then you can start putting hCG four weeks before the end. This should be done at 1000 IU every fourth day, five injections in total, and then stop.
 hCG Injection 12000 UI/Vial
hCG Injection 12000 UI/Vial
If the course is longer, from ten weeks or more, then the scheme changes a little. The fact is that the substance does not act in cells for long, about three days, and the cycle of division of sex cells also lasts about the same. It turns out that you need to maintain a more stable level of hCG. Again, these are observations and theory. In practice, it turns out that with long-term use of anabolics, it is better to administer hCG twice a week for five weeks and then take a break for two weeks.
The protocol for a long course looks like this: 5000 IU is needed for one cycle. We administer 500 IU twice a week for five weeks, then a break for two weeks. There are ten injections per cycle. If the course is not very long, and there is no nandrolone or trenbolone in it, then the break can be extended to a month.
A couple more important points. Firstly, Diluted HCG has not lost its properties for about a week. If you have a 5000 IU ampoule, you can divide it into five parts, dilute 1000 IU and administer 500 IU twice a week. With other concentrations, the principle is the same - divide and administer. Secondly, sodium chloride (saline) is used to dilute hCG. Usually, a dosage of 500 to 1500 IU is diluted in 1 ml of solvent.
- HCG course duration: Many experts recommend using gonadotropin during a long course of steroids (lasting more than 6 weeks).
Treatment: What to do if atrophy has already occurred
Unfortunately, already developed testicular atrophy often cannot be completely cured. In such cases, treatment is aimed at relieving symptoms and improving the quality of life.
- Testosterone replacement therapy (HRT). HRT is used to compensate for testosterone deficiency. This improves overall well-being, increases libido, increases muscle mass and strength.
- Assisted reproductive technologies (ART). In the absence of sperm, it may be necessary to use donor sperm to conceive a child.
Remember: a visit to an endocrinologist or urologist-andrologist specializing in men's health will help to significantly reduce health risks and optimize the use of pharmacology in training, if necessary. And remember this, friends! Our team specializes in supplying high-quality sports pharmacology throughout the United States and Europe. Therefore, you don't have to worry about quality from us. And with useful articles in the «Blog» section, you will definitely not be lost!
hCG protocols suggested by doctors Michael Scally and Eric Potratz1
If the course is short, only 5-6 weeks, and only one drug is used in small doses, then, according to these specialists, hCG is not necessary. But if the course is longer than 6 weeks (for example, 8-12 weeks), the dosages are higher, or a combination of two or more drugs is used, then it is worthwhile to play it safe. In this case, it is recommended to give two gonadotropin injections per week in the last 3-5 weeks of the course, 250-500 IU each, to prevent testicular atrophy. It is important to stop administering hCG after the anabolic drug is almost completely eliminated from the body, and only then begin post-cycle therapy.
If we are talking about multi-month courses, then the approach is slightly different. Gonadotropin is administered continuously, but in cycles: 3-5 weeks after 1-2 weeks of break. This break is needed to prevent so-called desensitization, when the testicles stop responding to hCG. According to the latest scientific data, this scheme is considered optimal, as it allows you to preserve the function of the testicles and promotes the most complete recovery after the course.
But what if hCG was not used during a long or «heavy» course? In this case, it can be included in the post-cycle therapy, but only at the very beginning of PCT. The so-called «blust protocol» from the book by William Llewellyns (Program for Wellness Restoration) is often used, which is also confirmed by clinical trials. According to this protocol, hCG is recommended to be used as part of PCT at 2000 IU every other day for 20 days to «restart» the hypothalamus-pituitary-testicles arc. But it is important to understand: such a scheme is highly discouraged unless there are complications. That is, if everything is going more or less normally, it is better to avoid it.
How do you know if the drug works at all? The only reliable indicator is a blood test for β-hCG. This test will show whether hCG really has the desired effect.
It is important to remember that hCG is not recommended for weight loss or to achieve an anabolic effect. This is a drug that is used to maintain testicular function during an anabolic steroid course.
Another important point that is often forgotten:
The size of the testicles is not always a reliable indicator of their work. The introduction of anabolic drugs leads to the suppression of luteinizing hormone, which maintains normal testicular function. After a 12–16-week AAS cycle, the volume of Leydig cells can decrease by 90%, and the secretion of natural testosterone - by 98%! But Leydig cells make up only about 5% of the testicle mass. Therefore, palpation analysis of the size of the testicles is not a reliable method of assessment, since the volume can change very slightly (only by 5%) with almost complete suppression of function.

Price of Human Chorionic Gonadotropin
Here, of course, the price range is quite large, and it depends mainly on what this hCG is needed for and in what form it is sold. The simplest option is home pregnancy tests. The price is small there, ranging from 1 to 15 dollars.
But if we are talking about injectable hCG, which is used to treat infertility or to maintain male health, then the numbers are different. A bottle with a dosage of 10,000 IU can cost from 50 to 80 dollars if you buy it at a pharmacy that makes prescription drugs and use a coupon. Well, and laboratory antigens, of course, will cost even more, hundreds of dollars.
In general, the price of hCG in the US varies widely, and depends on where and for what you buy it.
You can buy this drug at the best price directly on our website in the corresponding section of the catalog from the AnabolShop.org team!
We hope you enjoyed the article and thank you for reading.
Good anabolism to all athletes!
————————————————————
- http://www.steroidology.com/forum/anabolic-steroid-forum/143124-official-pct-2009-a.html#post2074469

Author: Alex Morozov
Alex Morozov is a strength training analyst and fitness culture researcher with over 12 years of experience in powerlifting, bodybuilding methodology, and performance optimization. He has worked with competitive athletes, studied training physiology, and analyzed long-term health outcomes related to strength sports.
Alex focuses on evidence-based training, athlete longevity, and realistic performance expectations. His work explores the psychological and cultural factors shaping modern fitness trends, including social media influence, enhancement debates, and recovery science.